The Master Guide to Age‑Related Macular Degeneration (AMD)
Age‑Related Macular Degeneration (AMD) is the leading cause of irreversible central vision loss in adults over 50, with global prevalence projected to approach 288 million people by 2040. Far from being an inevitable “wear and tear” consequence of aging, AMD is better understood as a localized manifestation of a systemic breakdown in lipid processing, iron balance, and chronic inflammation at the back of the eye.

This guide synthesizes the latest science as of 2026—covering pathophysiology, genetics, lifestyle, nutritional interventions (AREDS2 and beyond), complement and iron pathways, emerging bioactives such as saffron, and the rise of digital companions for long‑term retinal care.

1. The Macula and the Biological Engine Behind Sight
The macula is the small central zone of the retina that provides “high‑definition” vision for reading, recognizing faces, and seeing fine detail and color. Its unique performance comes at a cost: it operates under extremely high metabolic demand, high oxygen tension, and constant exposure to high‑energy visible light.
Three pressures make the macula uniquely vulnerable:
· High metabolic demand: Photoreceptors continuously convert light into neural signals, generating large amounts of metabolic waste.
· High oxygen tension: A rich oxygen supply supports this workload but also fuels reactive oxygen species (ROS), the “biological sparks” of oxidative damage.
· Constant light exposure: High‑energy blue light attacks polyunsaturated fatty acids (PUFAs) in photoreceptor membranes, promoting photo‑oxidative stress.
Behind the photoreceptors sits the Retinal Pigment Epithelium (RPE)—the eye’s essential “pit crew” that recycles shed photoreceptor segments, regulates nutrient flow, clears lipid waste, and produces antioxidants to neutralize ROS. Modern research places a special focus on Apolipoprotein M (ApoM), a protein that governs how effectively the RPE can “sweep away” harmful cholesterol and lipids via lysosomal lipid catabolism.
When this biological engine fails, AMD begins.

2. How AMD Develops: The Four Pillars of Decay
Contemporary models describe AMD as the progressive failure of the RPE–Bruch’s membrane–choriocapillaris complex driven by four interlocking molecular pillars.

2.1 Oxidative stress and retinal aging
The outer retina lives in a constant state of photo‑oxidative stress, with ROS attacking PUFA‑rich membranes and mitochondrial DNA. Over time this induces RPE senescence and a pro‑inflammatory secretory state that accelerates tissue damage.
2.2 Complement cascade and chronic inflammation
Genetic dysregulation of the alternative complement pathway is a hallmark of AMD. Variants such as the CFH Y402H polymorphism weaken Complement Factor H’s ability to regulate the cascade at the RPE–Bruch’s interface, allowing uncontrolled complement activation and formation of the Membrane Attack Complex (MAC) that punches holes in RPE cell membranes.
2.3 Lipid dysregulation and the ApoM/S1P axis
Lipotoxicity—accumulation of non‑esterified fatty acids and cholesterol—drives drusenogenesis, the formation of lipid‑rich deposits under the retina. The ApoM/S1P complex acts as a master regulator:
· Via S1PR3, it triggers RPE lysosomal lipid catabolism, enabling cells to sweep away cholesterol and prevent the “clogging” that precedes geographic atrophy.
· Via S1PR1, it maintains vascular barrier integrity, countering the leakage and neovascularization that define wet AMD.
Low circulating ApoM is increasingly seen as a systemic biomarker linking AMD to cardiometabolic disease, underscoring that the eye is not an island.
2.4 Iron homeostasis and ferroptosis
With aging, retinal iron levels can roughly double, fueling the Fenton reaction in which unbound iron reacts with hydrogen peroxide to generate highly reactive hydroxyl radicals. This drives ferroptosis, a regulated, iron‑dependent cell death pathway marked by lipid peroxidation and glutathione peroxidase 4 (GPX4) failure, now recognized as a major driver of RPE loss in geographic atrophy.
Clinical analyses link high‑dose oral iron (around 18–36 mg/day or more) in neovascular AMD to increased retinal or subretinal hemorrhage, especially in hypertensive patients, prompting caution around non‑indicated iron supplementation.

3. Clinical Types: Dry vs. Wet AMD
Although all AMD begins with metabolic stress and drusen formation, advanced disease follows two main pathways: a slow atrophic route (dry AMD) or a rapid exudative route (wet AMD).
|
Criteria |
Dry (Atrophic) AMD |
Wet (Neovascular) AMD |
|
Primary pathology |
Drusen accumulation; progressive RPE and photoreceptor loss leading to Geographic Atrophy (GA) |
Choroidal Neovascularization (CNV) with leaky, fragile vessels and subretinal fluid |
|
Progression speed |
Gradual; often over years or decades |
Rapid; vision can decline in days to weeks |
|
Visual impact |
Expanding central scotomas and loss of contrast sensitivity |
Distorted, wavy vision (metamorphopsia), sudden dark spots, and macular edema |
|
Prevalence |
80–90% of AMD cases |
About 10% of cases but ~90% of AMD‑related legal blindness |
|
Standard care (2026) |
AREDS2 for intermediate disease; complement inhibitors for GA |
Intravitreal anti‑VEGF agents (e.g., aflibercept 8 mg, faricimab) |

Metamorphopsia—straight lines appearing wavy or broken—is a critical warning sign of conversion from dry to wet AMD and should trigger urgent specialist evaluation.

4. Genetics and Lifestyle: Nature Meets Nurture
Twin and family studies suggest that roughly half or more of advanced AMD risk is attributable to inherited genetic factors, yet environmental choices powerfully modulate how quickly disease unfolds.
Key risk loci include:
· CFH (Complement Factor H): Variants (notably Y402H) impair complement regulation on host surfaces, increasing MAC‑mediated retinal injury.
· ARMS2/HTRA1: Strongly associated with progression to neovascular AMD and extracellular matrix remodeling under oxidative stress.
· C3 and CFI: Central complement components whose variants amplify chronic inflammation by making the cascade more “reactive” and harder to switch off.
These genes “load the gun,” but often remain silent until lifestyle triggers pull the proverbial trigger.


4.2 Modifiable environmental drivers
Major modifiable risk factors include:
· Smoking (roughly doubles risk; the single most important modifiable factor)
· High‑glycemic, low‑antioxidant diets
· Poor cardiovascular health (hypertension, obesity, atherosclerosis)
· Inadequate dietary intake of lutein, zeaxanthin, and omega‑3–rich fish
· Excess unprotected exposure to high‑energy visible and UV light
A Mediterranean‑style diet emphasizing leafy greens, colorful vegetables, and fatty fish is consistently associated with lower AMD incidence and slower progression.

4.3 Risk amplification and the intervention window
In individuals carrying high‑risk genotypes (for example CFH or ARMS2 variants), smoking and cardiometabolic stress do not simply add risk—they multiply it, leading to earlier failure of the RPE–Bruch’s membrane interface and more aggressive inflammation. The encouraging message is that lifestyle optimization can dampen high‑risk genetic signals and stretch the “therapeutic window” in which interventions are most effective.
5. Nutritional Interventions: From AREDS to Emerging Bioactives
5.1 AREDS and AREDS2: The evidence‑based standard
The National Eye Institute’s AREDS and AREDS2 trials established the first evidence‑based nutritional standard for AMD.
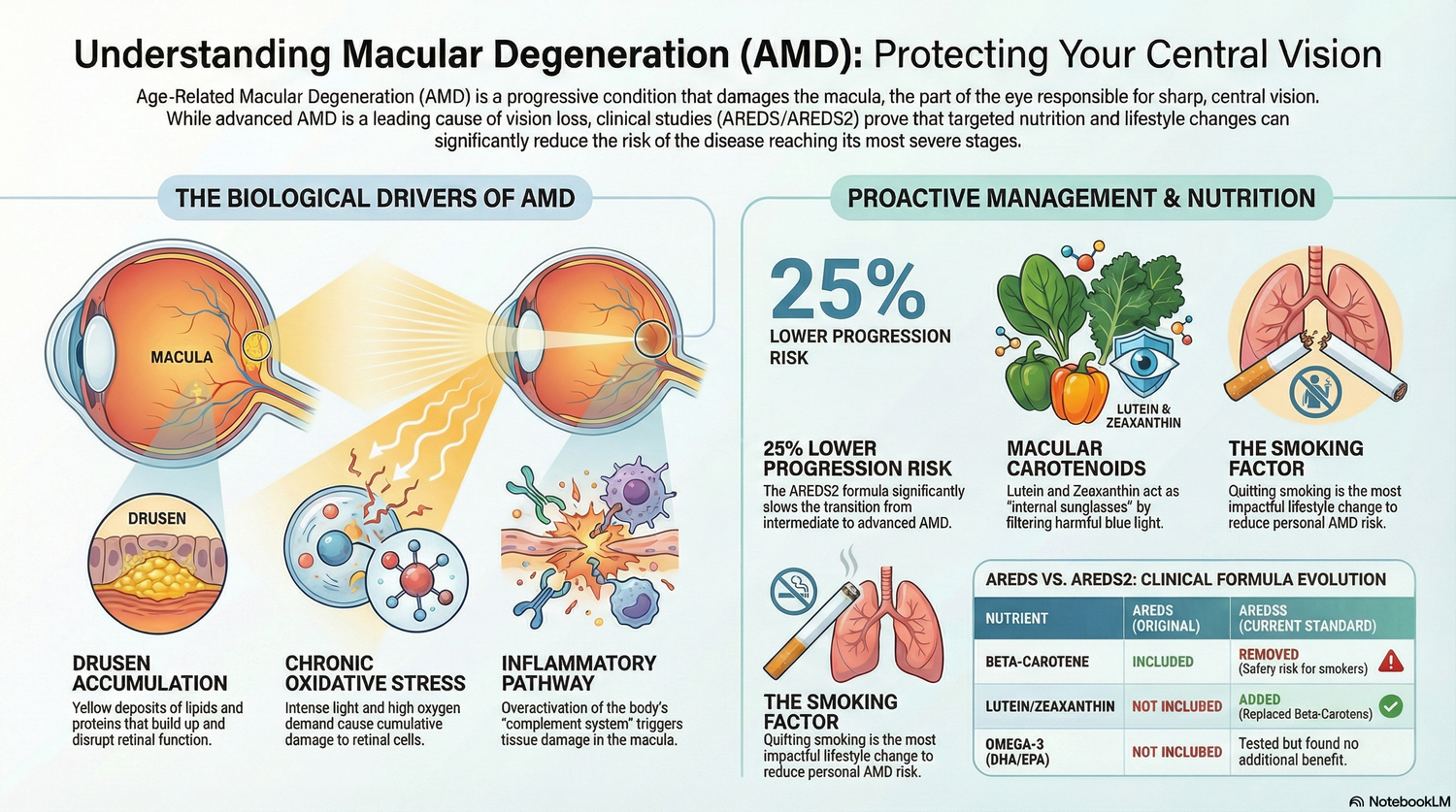
Key clinical finding: In individuals with intermediate AMD or advanced AMD in one eye, the original AREDS formulation reduced the 5‑year risk of progression to advanced AMD by about 25%. This benefit does not extend to people with only early changes or no AMD.
Formulation evolution
|
Nutrient |
Original AREDS |
AREDS2 (current standard) |
|
Vitamin C |
500 mg |
500 mg |
|
Vitamin E |
400 IU |
400 IU |
|
Zinc |
80 mg (zinc oxide) |
80 mg (or 25 mg in some variants, both effective) |
|
Copper |
2 mg (cupric oxide) |
2 mg (cupric oxide) |
|
Carotenoids |
15 mg β‑carotene |
10 mg lutein + 2 mg zeaxanthin (β‑carotene removed) |
|
Omega‑3s |
Not included |
Evaluated but ultimately excluded (no added benefit) |

Why β‑carotene was removed: Large trials showed β‑carotene nearly doubled lung cancer risk in current and former smokers, while lutein and zeaxanthin offered equal or better AMD protection without this safety concern.
5.2 The “Big Five” and macular pigment
The mechanistic synergy of AREDS2’s core nutrients underpins its clinical effect:
· Vitamin C and E: Work across aqueous and lipid phases to scavenge ROS; vitamin C helps regenerate oxidized vitamin E, preserving membrane integrity.
· Zinc (with copper): Cofactor for antioxidant enzymes like superoxide dismutase; copper prevents zinc‑induced anemia.
· Lutein and zeaxanthin: The only carotenoids that cross the blood‑retina barrier and concentrate in the macular pigment, acting as an internal “sunscreen” that filters blue light and quenches singlet oxygen.
Dietary sources with particularly high bioavailable macular carotenoids include cooked spinach and kale, egg yolks, orange peppers, and corn—especially when consumed with healthy fats to enhance absorption.

5.3 Saffron and resveratrol: Beyond structure to function
Recognizing AREDS2’s limitations—no benefit in early AMD and limited impact on iron and ApoM‑driven pathways—researchers have explored additional bioactives.
· Saffron (Crocus sativus): Clinical studies show improved retinal function and macular sensitivity in early‑to‑intermediate AMD, often measured by focal electroretinogram (fERG). Saffron is now integrated into multi‑pathway frameworks (such as “AMD‑11”) as a neuroprotective adjunct to AREDS2.
· Resveratrol: Acts as a metabolic and anti‑inflammatory modulator, protecting RPE cells from oxidative injury and suppressing the senescence‑associated secretory phenotype (SASP).
These agents aim to preserve function (sensitivity and performance) rather than only slowing structural decay, positioning them as promising tools for early AMD where AREDS2 alone falls short.
6. Complement Inhibitors, Iron Risk, and Future Therapeutics
6.1 Complement inhibitors for geographic atrophy
Two intravitreal complement inhibitors now offer the first disease‑modifying therapy for GA:
· Pegcetacoplan (C3 inhibitor): Roughly 16–22% GA growth reduction at 24 months, with up to around 42% reduction in some non‑subfoveal subgroups at 36 months.
· Avacincaptad pegol (C5 inhibitor): Approximately 14–18% GA growth reduction at 12 months, with long‑term data up to about 40% reduction.
Both agents carry a non‑trivial risk of exudative conversion to wet AMD (on the order of 1–21%, depending on regimen and baseline risk), underscoring the need for vigilant monitoring and patient‑specific risk‑benefit discussion.
6.2 Iron and the “retinal villain” paradox
While essential for energy metabolism, excessive iron acts as a retinal toxin by driving ferroptosis and promoting hemorrhage risk in neovascular AMD. Current guidance is to avoid high‑dose iron supplements in AMD patients unless clearly indicated for confirmed iron‑deficiency anemia and managed in coordination with both ophthalmology and primary care.
6.3 ApoM‑based and gene therapies on the horizon
Engineered ApoM‑Fc constructs have demonstrated preclinical efficacy in attenuating CNV and improving RPE lipid handling, hinting at future systemic therapies that address the underlying lipid‑processing failure shared by AMD and cardiovascular disease. Parallel pipelines include one‑time gene therapies and more targeted complement modulation that may further personalize care in the coming decade.
7. Monitoring, Symptoms, and the Role of Digital Companions
7.1 Early symptoms and functional biomarkers
Because early AMD is often asymptomatic on standard visual acuity charts, functional cues are critical:
· Metamorphopsia (wavy or broken lines)
· Central blur or new dark spots
· Difficulty with dark adaptation (for example in dim restaurants or night driving)
Home tools such as the Amsler grid and smartphone‑based dark adaptation (DA) tests now complement clinic visits. Metrics like Area Under the Dark Adaptation Curve (AUDAC) and Rod Intercept Time (RIT) can distinguish AMD eyes from age‑matched controls even when visual acuity remains 20/20.
7.2 Digital health coaching and voice‑first interfaces
AMD is a chronic, multi‑pathway disorder, but traditional care remains episodic. Digital health technologies are closing this gap by providing continuous, behaviorally informed support.
Key findings:
· Intelligent Voice Assistants (IVAs): In seniors, voice‑first systems have increased Medication Possession Ratios (MPR) from about 62% to 87%, with users averaging several interactions per day.
· Digital coaching platforms: Demonstrate meaningful reductions in fasting glucose and weight, and large gains in eHealth literacy, translating into improved adherence and self‑efficacy.
· Psychological benefits: Reductions in depression, health distress, and anxiety around disease management are repeatedly documented and strongly linked to sustained engagement.
For AMD specifically, voice‑first “retinal companions” aligned with the Geriatrics 5Ms (Medications, Mind, Mobility, What Matters Most, Multicomplexity) offer an accessible way to manage complex regimens like AREDS2, complement injections, and cardiometabolic therapies without relying on impaired central vision.

8. Practical Takeaways for Patients and Clinicians
From the integrated 2026 evidence base, a few practical principles emerge:
· AMD is a systemic metabolic disease with a retinal “face,” tightly linked to lipid processing, iron balance, complement genetics, and cardiovascular health.

· AREDS2 remains foundational for intermediate AMD or advanced AMD in one eye, not for primary prevention or very early disease.
· Saffron and related bioactives show added functional benefits in early‑to‑intermediate AMD and may complement, but not replace, AREDS2.
· High‑dose iron is potentially hazardous in AMD—particularly neovascular AMD—and should only be used when clearly indicated and monitored.
· Complement inhibitors offer meaningful slowing of GA but require careful monitoring for exudative conversion.
· Voice‑first, digital companion ecosystems are emerging as a critical third pillar alongside pharmacology and nutrition, especially for older adults with central visual distortion.

For a brand like Persavita, the strategic message is clear: protecting vision in AMD demands a multi‑pathway, multi‑modal framework that integrates targeted nutrition, systemic metabolic health, precision biologics, and accessible digital coaching tools tailored to the realities of aging eyes.








{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.